BPC-157 vs TB-500: How They Compare for Healing
BPC-157 and TB-500 are the two most-discussed healing peptides. Here's how they actually compare on mechanism, evidence, dosing, side effects, and which one (or both) makes sense for which goal.
By PeptidesDB EditorialPublished Jun 14, 20267 min read
BPC-157 and TB-500 are the two most-cited research peptides for soft-tissue healing. They work through partially overlapping but distinct mechanisms, have different evidence bases (animal-heavy for both, with TB-500 having one completed Phase 2 human trial in a different indication), and are often stacked rather than chosen one-or-the-other. Below is a side-by-side and a practical decision frame.
Quick verdict table
| BPC-157 | TB-500 (Thymosin Beta-4 fragment) | |
|---|---|---|
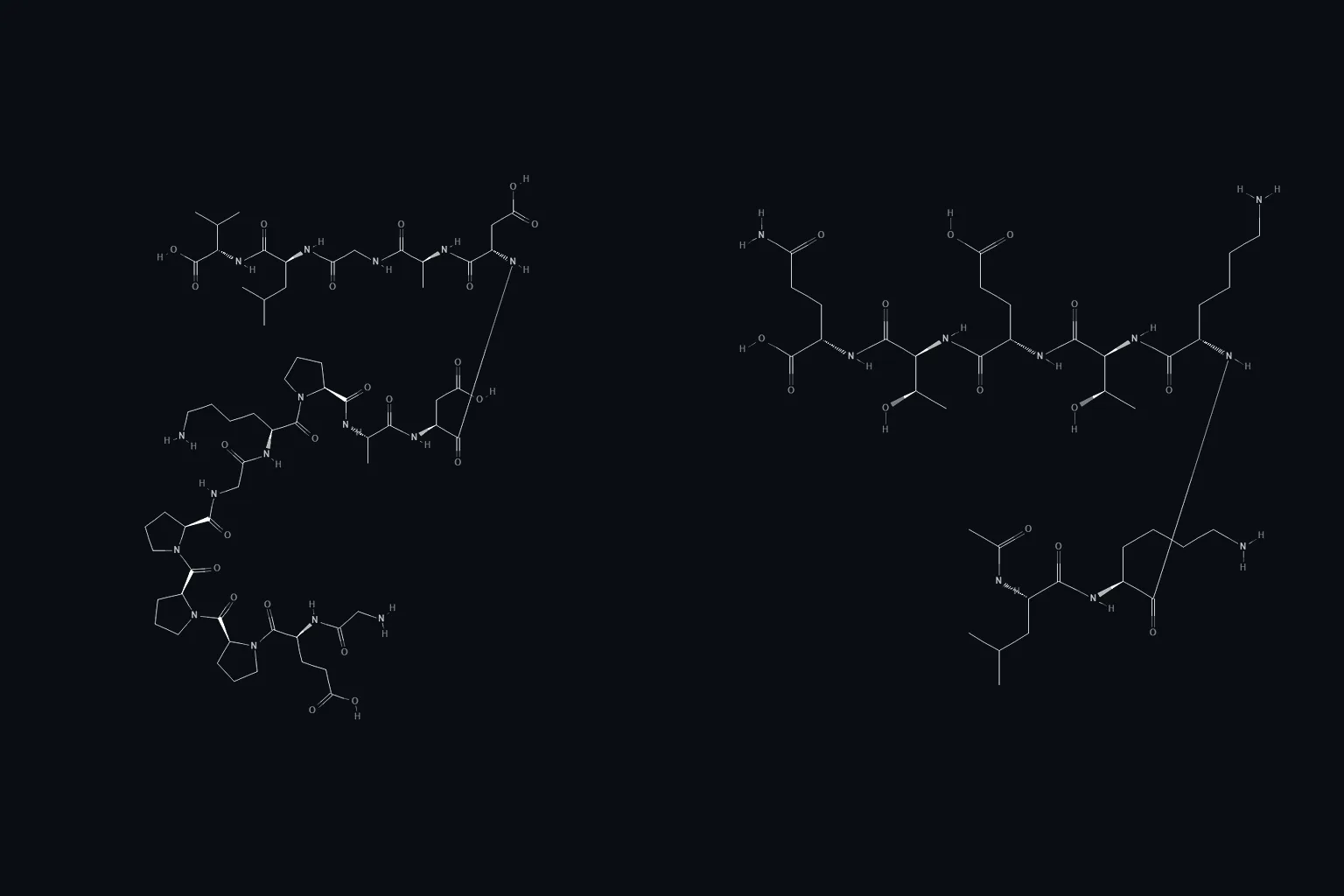
| What it is | 15-amino-acid synthetic pentadecapeptide derived from a gastric protein | Synthetic short fragment of Thymosin Beta-4 (Ac-LKKTETQ) |
| Primary mechanism | Upregulates VEGF; angiogenesis; nitric-oxide pathway; tendon-fibroblast growth | G-actin sequestration; cell migration; angiogenesis; modulates inflammation |
| Best-studied indications | Tendon and ligament repair, GI lining, muscle tear recovery, gut inflammation | Wound closure, dry-eye disease (Phase 2), tissue migration after injury |
| Form | Subcutaneous injection (most common); oral has some animal data, less in humans | Subcutaneous injection |
| Typical dosing in literature | 250–500 mcg per dose, daily or BID, 4–8 week cycles | 2–2.5 mg twice weekly to weekly, 4–6 week loading; lower maintenance |
| Onset of subjective effect | Days to ~2 weeks for soft-tissue cases | 1–3 weeks |
| Half-life | Short (~minutes) but downstream effects persist | Modest (hours) for the fragment |
| Human evidence quality | Many small case series; no completed Phase 3 in humans | One completed Phase 2 in dry eye; otherwise animal-heavy |
| Common side effects | Mild; occasional injection-site irritation, transient lightheadedness | Mild; occasional injection-site irritation, fatigue at high doses |
| Often stacked with | TB-500, GHK-Cu | BPC-157, GHK-Cu |
| PeptidesDB profile | BPC-157 | TB-500 |
What each peptide actually is
BPC-157
BPC-157 (Body Protection Compound-157) is a 15-amino-acid sequence isolated from a larger gastric protein found in human gastric juice. Synthesized for research in the early 1990s, it's been studied in dozens of rodent injury models — Achilles tendon transection, muscle laceration, ligament rupture, stress-ulcer models, colitis models. The animal literature is extensive and unusually consistent in showing accelerated healing across tissue types.
The leading mechanism story: BPC-157 upregulates VEGF (vascular endothelial growth factor), which drives angiogenesis (new blood-vessel growth into injured tissue), and influences the nitric-oxide pathway in vascular endothelium. It also appears to directly increase tendon-fibroblast outgrowth and migration in cell-culture studies. The net effect in animal injury models: faster collagen organization, faster gross healing, less scar.
Human data is currently dominated by small case series and observational reports. There is no completed Phase 3 trial. A handful of small clinical studies have looked at inflammatory bowel and ulcer indications with positive but underpowered results. The FDA tightened the 503A compounding list in 2023, removing BPC-157 from the list of peptides compounding pharmacies could legally provide, which is a regulatory rather than safety judgment.
TB-500
TB-500 is a synthetic short fragment of Thymosin Beta-4 — a 43-amino-acid actin-binding protein found in essentially every mammalian cell type. The most commonly sold "TB-500" is actually the active 4-amino-acid peptide region (Ac-LKKTETQ), not the full Thymosin Beta-4 molecule. Full Thymosin Beta-4 has been in human clinical trials for wound healing, dry eye, and cardiac repair; the fragment has been used in animal-injury and racehorse settings for years.
Mechanism: Thymosin Beta-4 sequesters G-actin (the monomer form of the cytoskeletal protein actin), regulating cell migration and tissue assembly. In injury contexts, that translates to faster recruitment of stem cells and endothelial cells to the wound site, faster angiogenesis, and modulated inflammation. The fragment shares many but not all of the parent protein's biological activities.
The strongest human evidence is from a Phase 2 dry-eye trial that completed successfully (Ribrelan / RGN-259). For musculoskeletal healing, the human evidence is mostly case series and athlete-community reports.
Mechanism overlap and complementarity
Both peptides drive angiogenesis. Both modulate inflammation. Both have been shown in animal models to speed soft-tissue repair. The mechanisms are not identical:
- BPC-157 primarily works through VEGF / nitric-oxide / fibroblast biology — the building and connecting side of tissue repair.
- TB-500 primarily works through actin / cell-migration biology — the getting cells to the right place side of tissue repair.
This is the rationale for the common "BPC-157 + TB-500" stack — informally called the Wolverine Stack. The hypothesis is that the two peptides hit different limiting steps in the healing cascade and produce additive effects. Direct head-to-head data testing this hypothesis in humans does not exist; it's plausible based on mechanism but not proven.
Side effects and safety
Both peptides have favorable acute-safety profiles in the published data. The most-reported issues are mild and not specific to either compound: injection-site irritation (often a site-rotation or solvent issue, not the peptide itself), transient lightheadedness in the first few doses, mild fatigue. Allergic reactions are rare but possible.
Long-term safety in humans is unstudied for both. The chronic-dose question — what happens after a year of continuous use — does not have a published answer for either peptide. This is the primary reason most users cycle these peptides (4–8 week courses with rest periods) rather than dose continuously.
For the full safety frame, see are peptides safe?.
Dosing patterns from the literature
BPC-157 dosing
The most-cited research dosing is 250–500 mcg per dose, once or twice daily, for 4–8 weeks for soft-tissue indications. Subcutaneous injection is the default route. Oral dosing has some animal data showing local effects in the GI tract; systemic effects from oral dosing in humans are less clear.
For dose math, see the reconstitution calculator. A typical reconstitution: 5 mg vial in 2 mL BAC water → 2.5 mg/mL → 250 mcg = 10 units on a U-100 insulin syringe.
TB-500 dosing
The typical research dosing is heavier and less frequent: 2–2.5 mg twice weekly during a 4–6 week "loading" phase, then 2–2.5 mg weekly for a 4–6 week "maintenance" phase. Subcutaneous injection.
For dose math: a 5 mg vial in 2 mL BAC water → 2.5 mg/mL → 2.5 mg = 100 units on a U-100 syringe (a full 1 mL barrel). Most users prefer to reconstitute TB-500 with less BAC water (e.g., 5 mg in 1 mL → 5 mg/mL → 2.5 mg = 50 units) so the per-dose volume is more practical.
Which to choose
A practical frame:
- Tendon or ligament injury (Achilles, rotator cuff, plantar fascia, etc.). BPC-157 is the more direct match to the animal-injury literature. Many users add TB-500 as a 4–6 week loading-phase add-on.
- Acute muscle tear or strain. BPC-157 has the most-cited animal data for muscle laceration. Healing window is often weeks.
- Surgical recovery. Often the Wolverine Stack (BPC-157 + TB-500 + sometimes GHK-Cu) is referenced; the rationale is mechanism complementarity. Always discuss with the surgical team — peptide-effects on surgical-site biology are not well-characterized clinically.
- GI inflammation or ulcers. BPC-157 has the most direct rationale based on the source protein and animal data; consult a GI specialist.
- Dry eye or other epithelial-repair indications. TB-500 (or full Thymosin Beta-4) has the most direct rationale based on the completed Phase 2 trial.
The stack option (BPC-157 + TB-500)
The two are commonly combined. A representative pattern from community usage:
- BPC-157 250 mcg twice daily, daily for 4–6 weeks.
- TB-500 2.5 mg twice weekly for 4 weeks, then 2.5 mg weekly for 4 weeks.
- Both subcutaneous, rotate injection sites; see where to inject peptides.
Head-to-head trials comparing stack vs monotherapy do not exist. The rationale is mechanism complementarity, not proven additive effect.
Bottom line
- Both peptides have strong animal-injury data, modest human data, mild acute side-effect profiles, and unstudied long-term safety.
- BPC-157 is the more direct match to most soft-tissue injury patterns based on the literature.
- TB-500 has a stronger fit for epithelial-repair indications and is often added as a stack partner for soft-tissue recovery.
- The stack is common in practice; the case for it is mechanistic, not yet evidence-based at trial-data level.
Per-peptide research profiles with full citations: BPC-157, TB-500. For practical operating guides: how to reconstitute peptides, how to inject peptides. For the safety frame: are peptides safe?.